
Salivary gland infections are most commonly caused by dehydration, poor oral hygiene, smoking, dry mouth (xerostomia), blocked salivary ducts (salivary stones), a weakened immune system, and recent dental or oral procedures. Most cases are preventable with simple daily habits, and early treatment by an ENT specialist gives the best outcomes.
If you have ever felt a painful swelling below your ear or under your jaw after eating, especially after biting into something sour, you may have experienced what a salivary gland infection feels like. It is more common than most people realise, and it can affect anyone.
Salivary glands play an important role in keeping your mouth healthy. They produce saliva that keeps your mouth moist, helps you chew and swallow, and protects your teeth and throat from harmful bacteria. When they get infected, a condition medically called sialadenitis , the results can range from mildly uncomfortable to severely painful.
As an ENT specialist in Nashik, I have treated many patients who had no idea what triggered their infection. Understanding the risk factors is the first step toward prevention.
What Is a Salivary Gland Infection?
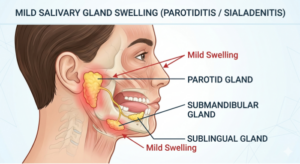
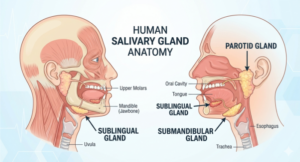
A salivary gland infection occurs when bacteria or viruses invade one of your three major salivary glands, the parotid (near your cheeks), submandibular (under your jaw), or sublingual (under your tongue). The parotid and submandibular glands are most commonly affected.
Common symptoms include swelling and tenderness in the face or neck, pain while eating, difficulty opening your mouth, a foul taste or pus discharge, and fever in more severe cases. Studies suggest that acute bacterial sialadenitis accounts for a significant portion of head and neck infections seen in ENT clinics, particularly in older adults and hospitalised patients.
Top 7 Risk Factors for Salivary Gland Infection
1. Dehydration: The Most Overlooked Trigger
This is by far the most common and most preventable risk factor. When your body does not have enough water, your salivary glands produce less saliva. Saliva is your mouth’s natural defence system, it flushes out food particles and bacteria. Without adequate saliva flow, bacteria multiply quickly in the ducts and gland tissue.
Think about patients who come in during peak summer months, or those recovering from illness who are not drinking enough fluids. Even a day or two of poor hydration can increase your risk. Hospital patients on restricted oral intake are especially vulnerable, which is why nurses often remind them to keep their mouth moist.
Simple Tip: Drink at least 8–10 glasses of water every day. If you are unwell or fasting, keep sipping small amounts of water frequently. This one habit alone can significantly reduce your risk.

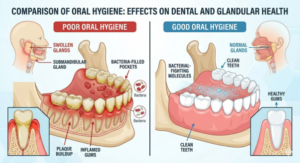
2. Poor Oral Hygiene: Bacteria’s Open Invitation
Your mouth is home to hundreds of bacteria, most of them harmless. But when you do not brush regularly, skip flossing, or neglect dental visits, harmful bacteria accumulate along the gum line, teeth, and salivary duct openings. These bacteria can travel up the ducts into the glands, causing infection.
Staphylococcus aureus is one of the most common bacteria found in acute salivary gland infections, and it often originates from within the oral cavity itself. Patients who use dentures, have cavities, or suffer from gum disease are at higher risk because the bacterial load in their mouth is already elevated.
Simple Tip: Brush your teeth twice a day, floss daily, use an antibacterial mouthwash, and visit your dentist every six months. Good oral care is not just about your teeth, it protects your entire throat and glandular system.
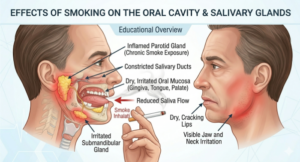
3. Smoking and Tobacco Use: Drying Out More Than Your Lungs
Smoking and chewing tobacco are damaging in many ways that most people know about, but their effect on salivary glands often goes unnoticed. Tobacco reduces saliva production, impairs the immune response of the gland’s lining, and increases the concentration of bacteria inside the mouth.
Chronic smokers are significantly more prone to sialadenitis and also face a higher risk of salivary gland tumours over time. ENT specialists often note that tobacco users present with recurrent or more severe infections compared to non-smokers. If you use bidi, cigarettes, or any tobacco product, this is one more reason to consider quitting.
Simple Tip: Seek support to quit tobacco. Nashik has tobacco cessation helplines and ENT clinics can guide you on managing withdrawal symptoms
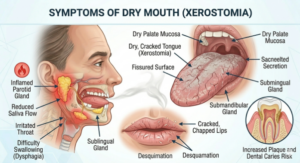
4. Dry Mouth (Xerostomia) from Medications: A Hidden Side Effect
Many commonly prescribed medications cause dry mouth as a side effect. Antihistamines (allergy tablets), antidepressants, diuretics (water tablets), blood pressure medications, and certain psychiatric drugs all reduce saliva flow. This may seem like a minor annoyance, but it significantly raises the risk of salivary gland infection.
Older adults are particularly affected because they are often on multiple medications simultaneously, a situation called polypharmacy. If you take regular medications and have noticed persistent dry mouth, do mention it to your doctor. There are saliva substitutes and oral rinses that can help manage this.
Simple Tip: Tell your ENT or physician if your mouth feels chronically dry. Do not stop any medication on your own, but ask about alternatives or supportive treatments for xerostomia.
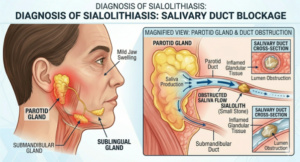
5. Salivary Duct Blockages (Salivary Stones / Sialolithiasis)
Salivary stones are small, hard deposits, made of calcium and other minerals, that form inside the salivary ducts. When they block the duct, saliva cannot flow freely. This creates a backup, and the stagnant saliva becomes a breeding ground for bacteria, leading to infection.
Sialolithiasis most commonly affects the submandibular gland (the gland under your jaw) and tends to be more common in middle-aged adults. The classic symptom is a sharp, colicky pain that appears when you eat, especially when you anticipate food or bite something sour — and then slowly subsides. If left untreated, recurrent blockages lead to chronic infections and gland damage.
Simple Tip: If you regularly notice swelling under your jaw during meals, do not ignore it. A simple ultrasound scan can detect salivary stones early, and most cases are treatable without major surgery.
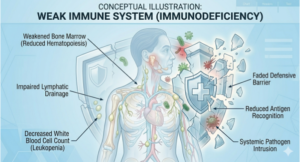
6. Weakened Immune System: When Your Defences Are Down
People with diabetes, HIV, cancer (especially those undergoing chemotherapy or radiation to the head and neck), autoimmune conditions, or those on long-term steroid therapy are at much higher risk for salivary gland infections. When the immune system is compromised, the body struggles to fight off even common bacteria that would otherwise be harmless.
Diabetic patients in particular face a double challenge: high blood sugar levels create an ideal environment for bacterial growth, and diabetes-related nerve and blood vessel damage can impair the gland’s ability to fight infection. ENT doctors always consider an underlying systemic condition when a patient presents with recurrent or unusually severe salivary gland infections.
Simple Tip: Managing your underlying condition, whether diabetes, autoimmune disease, or another chronic illness, is the most effective way to reduce infection risk. Regular health check-ups are key.
7. Recent Dental or Oral Procedures: A Temporary but Real Risk
Dental extractions, oral surgeries, endoscopies, or the placement of dentures and oral appliances can temporarily disturb the normal bacterial environment of the mouth. Bacteria introduced during or after the procedure ,combined with inflammation and reduced salivary flow can create conditions that allow the salivary glands to become infected.
Patients who are on nothing-by-mouth (NPO) status before and after surgery, or those with a nasogastric tube, are also more vulnerable because their normal salivary flow is disrupted. This type of hospital-acquired salivary gland infection is known as acute suppurative parotitis and is well-documented in surgical literature.
Simple Tip: After any dental or oral procedure, follow your post-care instructions carefully, stay hydrated, and maintain gentle oral hygiene. If you notice facial or neck swelling in the days following a procedure, see your doctor promptly.
When to Visit an ENT Doctor in Nashik?
Most people wait too long before seeking help for salivary gland problems. They assume the swelling will go away on its own and sometimes it does. But there are clear warning signs that mean you should see an ENT specialist without delay.
Book an appointment if you notice:
- A swelling near your jaw, cheek, or neck that is getting larger or not going away after 2–3 days
- Pain while eating, especially when anticipating food or tasting something sour
- A foul taste or visible pus in your mouth near the gland opening
- Fever along with facial swelling — this can indicate an abscess that needs urgent care
- Multiple episodes of similar swelling in the past (recurrent infection is also a sign)
- A hard lump in the area that does not go away (needs evaluation to rule out a salivary stone or tumour)
At Dr. Sudarshen Aahire’s ENT clinic in Nashik, patients with salivary gland concerns receive a thorough clinical examination, ultrasound guidance when needed, and a personalized treatment plan. Whether the problem is a simple infection, a salivary stone, or a recurring condition, early diagnosis always leads to simpler and faster recovery.
If you notice persistent swelling, pain during meals, or a foul taste that does not go away, do not wait it out. A quick visit to an ENT specialist can confirm the diagnosis, prevent complications, and get you back to eating and speaking comfortably.
Frequently Asked Questions
Q1: What are the first signs of a salivary gland infection?
The earliest signs are usually pain and swelling near your cheek, jaw, or under your chin often worsening when you eat. You might also notice a dry or bad taste in your mouth. If the infection progresses, you may develop fever and difficulty opening your mouth.
Q2: Can a salivary gland infection go away on its own?
Mild cases may improve with good hydration, warm compresses, and improved oral hygiene. However, bacterial infections usually require antibiotic treatment. Never ignore a worsening swelling or fever; these need urgent medical evaluation to rule out an abscess.
Q3: What is the most common cause of salivary gland infections?
Dehydration reducing saliva flow is the leading cause, followed by poor oral hygiene and salivary duct blockages (stones). In hospitalised patients, bacteria from the mouth travelling up dry salivary ducts is the most frequent mechanism.
Q4: Are salivary gland infections contagious?
No, bacterial salivary gland infections (sialadenitis) are not contagious. However, viral causes such as the mumps virus are contagious and spread through saliva and respiratory droplets. The MMR vaccine protects against the viral form.
Q5: Who is most at risk for recurring salivary gland infections?
People with salivary stones, chronic dry mouth, diabetes, immune deficiencies, or a habit of smoking are most prone to recurring infections. Recurrent episodes should always be evaluated by an ENT specialist to identify and address the underlying cause.
Q6: How is a salivary gland infection diagnosed?
An ENT doctor will examine the gland clinically and may order an ultrasound to check for stones, abscess formation, or gland enlargement. In some cases, a CT scan or fine-needle aspiration may be needed to rule out other conditions like tumours.
Q7: Is surgery required to treat salivary gland infections?
Most infections respond well to antibiotics and supportive care — including hydration, warm compresses, and massaging the gland. Surgery is only needed when there is an abscess that needs drainage, a stone that cannot pass naturally, or a chronically damaged gland.
Q8: Can children get salivary gland infections?
Yes, children can develop salivary gland infections, most commonly from the mumps virus if unvaccinated. Juvenile recurrent parotitis is another condition seen in children with repeated episodes of parotid swelling. Any persistent facial swelling in a child should be evaluated by a paediatrician or ENT specialist.
Dr. Sudarshen Aahire is a young, talented, and vibrant ENT and Pediatric doctor in Nashik with 12 years of experience. Apart from routine ENT care and surgeries he specializes in the management of Snoring and obstructive sleep apnea surgeries, Endoscopic skull base surgeries, voice-related disorders, and voice surgeries, airway and swallowing disorders.