Key Takeaways
- More than 80% of people who believe they have a sinus headache are actually experiencing migraine.
- A true sinus headache brings steady facial pressure with nasal discharge, congestion, and reduced sense of smell.
- Migraine pain throbs, often one-sided, with nausea and light sensitivity, and lacks nasal congestion or discharge.
- Trigeminal neuralgia causes brief, electric-like facial pain triggered by speaking, eating, or light touch.

A dull ache across the forehead. That heavy, stuffed-up feeling behind the cheeks. Pain that seems to radiate from somewhere inside the face. When these sensations show up, most people arrive at the same conclusion: it must be the sinuses.
That instinct is understandable -but it’s frequently incorrect. A striking number of people who self-diagnose a sinus problem are, in fact, experiencing something else entirely. Treating the wrong condition doesn’t just fail to help; it delays the care that would actually work.
What happens inside the sinuses during an infection
Under healthy conditions, the sinuses -hollow spaces distributed across the face and skull -remain clear and well-ventilated. An infection disrupts this balance. Inflamed tissue narrows the drainage pathways, mucus has nowhere to go, and the resulting pressure builds against the walls of the sinus cavities. That pressure is what registers as facial pain.
A true sinus headache has a recognisable profile. The discomfort tends to be steady rather than pulsating, concentrated around the forehead, cheekbones, and the area beneath the eyes. But it almost never appears in isolation. Accompanying signs typically include:
- Thick nasal discharge, often yellow or green
- Significant nasal congestion making breathing difficult
- Facial pain that deepens when the head is tilted forward
- A dulled or absent sense of smell
- Low-grade fever in some presentations
The takeaway: if the nose is clear and there’s no discharge, the sinuses are unlikely to be the source of the problem.
What Else Can Cause Facial Pain? Understanding Similar Conditions
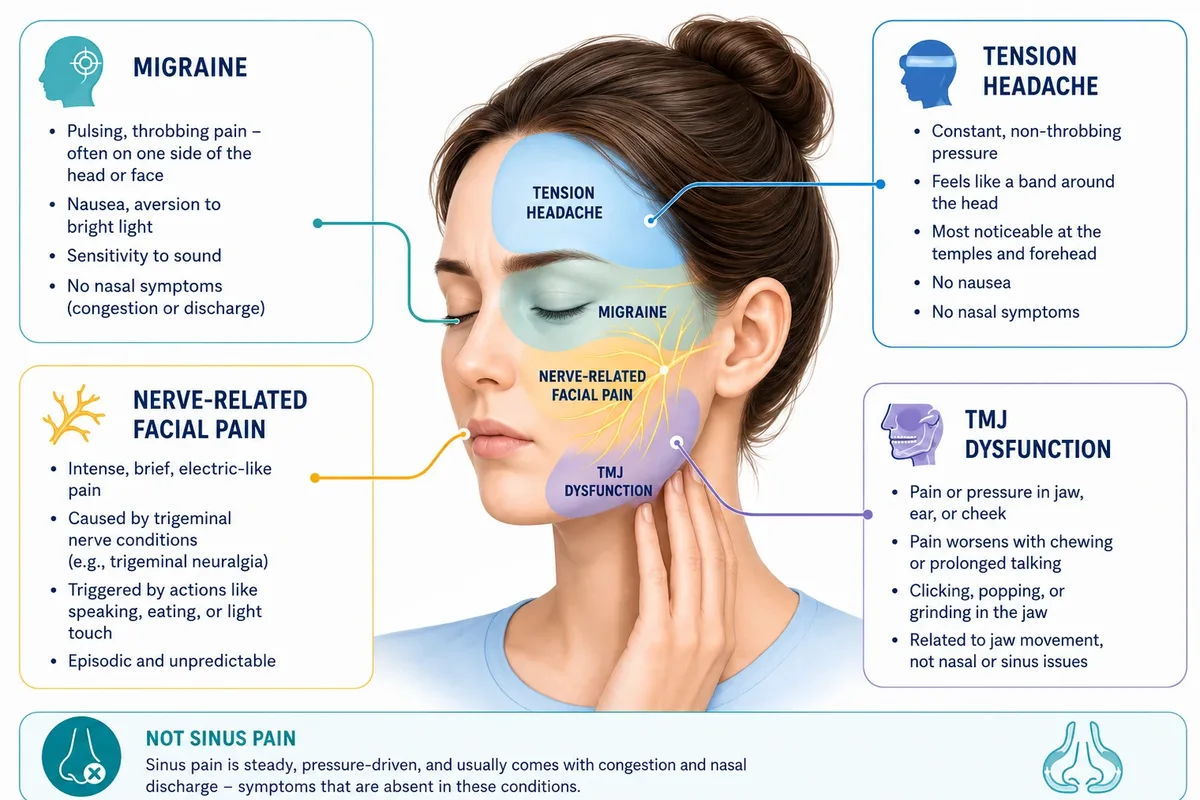
Migraine
Migraine stands apart from sinus headache in several important ways, though the two can feel deceptively similar in the early stages. Where sinus pain is steady and pressure-driven, migraine pain tends to pulse and throb -often on one side of the head or face rather than both. Nausea, an aversion to bright light, and heightened sensitivity to sound are hallmarks of migraine that simply don’t feature in sinus headache. The absence of nasal symptoms is the most reliable distinguishing clue: migraines don’t produce the congestion and discharge that go hand-in-hand with sinusitis.
Tension headache
When stress, fatigue, or sustained muscle tension leads to a headache, the result is typically a constant, non-throbbing pressure that wraps around the head -most noticeably at the temples and across the forehead. It doesn’t worsen with movement, doesn’t cause nausea, and has no nasal component. The pain is present but comparatively flat, without the escalating quality of migraine or the deep facial ache of sinusitis.
Nerve-related facial pain
Conditions affecting the trigeminal nerve -the primary sensory nerve of the face -can generate intense, unpredictable pain that has little in common with a sinus headache once properly examined. Trigeminal neuralgia is characterised by brief but severe episodes of sharp, electric-like pain, frequently ignited by ordinary actions such as speaking, eating, or a gentle touch to the face. The episodic, triggered nature of this pain distinguishes it clearly from the sustained pressure of a sinus complaint.
Temporomandibular joint (TMJ) dysfunction
The joint connecting the jaw to the base of the skull sits close enough to the ear and cheek region that inflammation there can register as facial pressure. Patients with TMJ dysfunction often notice that their pain flares during meals or after prolonged talking, and may detect an audible clicking or grating in the jaw. These clues -linked to jaw movement rather than breathing or nasal function -point away from the sinuses entirely.
How ENT & TMJ Specialists Differentiate Facial Pain Conditions
| Feature | True sinus headache | Migraine |
| Nasal symptoms | Nearly always present | Generally absent |
| Character of pain | Constant, pressure-like ache | Pulsating or throbbing |
| Typical location | Forehead, cheeks, under eyes | One side of head or face |
| What sets it off | Bacterial or viral infection | Hormones, triggers, stress, light |
| Additional signs | Fever, discharge, smell changes | Nausea, light and sound sensitivity |
| Episode pattern | Tied to active illness | Recurs independently of illness |
Why the wrong diagnosis keeps happening
Facial pain doesn’t come with a label. The overlap between conditions -especially migraine and sinusitis -is enough to fool both patients and, at times, clinicians who don’t specialise in this area. Several patterns make misdiagnosis particularly common:
- Pain location drives the assumption -forehead or cheek pain feels like a sinus problem regardless of what’s actually causing it
- Over-the-counter sinus remedies sometimes reduce general inflammation and offer brief relief, which reinforces the wrong conclusion
- Without nasal endoscopy or imaging, structural causes can be entirely invisible to a standard examination
- Patients often don’t mention associated symptoms like nausea or light sensitivity because they don’t connect them to the facial pain
How an ENT specialist approaches the evaluation
An ENT evaluation moves beyond location-based guesswork. The aim is to establish whether actual sinus disease is present -not simply to treat the area where pain is felt.
This may involve direct examination of the nasal passages, assessment of sinus drainage pathways, and imaging where the clinical picture isn’t definitive. Only once sinus involvement is confirmed -or ruled out -does a targeted treatment plan take shape.
Dr. Sudarshan Aahire applies this structured diagnostic approach to ensure that patients receive care matched to their actual condition, not a best guess based on symptom location alone.
Signs That an ENT Appointment Is the Right Next Step
Consider specialist evaluation with Dr. Sudarshen Aahire if you’re experiencing any of the following:
- Recurrent facial pain that returns even after completing treatment
- Congestion and thick nasal discharge accompanying your headaches
- A noticeable decline in your ability to smell
- Headaches that haven’t responded to standard pain relief
- Facial pressure present for more than 10 days without improvement
Key takeaways
- Facial pressure is a symptom, not a diagnosis -its location doesn’t confirm a sinus cause
- Migraine accounts for the majority of headaches that patients label as sinus-related
- Nerve pain, jaw dysfunction, and tension headaches can all present with facial discomfort
- Nasal symptoms -discharge, congestion, smell loss -are the clearest indicators of genuine sinusitis
- Specialist evaluation replaces guesswork with a treatment plan that actually fits the condition
Frequently asked questions
1. How intense can sinus headache pain get?
When the sinuses are significantly blocked and inflamed, the built-up pressure can cause considerable pain -particularly across the forehead and below the eye sockets. That said, very severe or one-sided pain with nausea warrants evaluation for migraine rather than sinus disease.
2. What is the most practical way to distinguish between the two?
Pay attention to what else is happening. A sinus headache almost always involves congestion and nasal discharge. A migraine typically involves throbbing pain, sensitivity to light and sound, and nausea -without significant nasal symptoms.
3. Why does tilting the head forward make things worse?
Forward movement shifts the fluid sitting in blocked sinus cavities, momentarily increasing the pressure against the sinus walls -which amplifies the pain. This effect is specific to sinus-related headaches and not typical of migraine.
4. Can a sinus headache occur without any nasal congestion?
It’s uncommon. True sinusitis almost always produces some degree of nasal involvement. Facial pain in the absence of any nasal symptoms is much more likely to have a non-sinus origin and deserves investigation accordingly.
5. Is imaging always required for diagnosis?
Not in straightforward cases. Clinical examination and symptom history are often sufficient. However, when symptoms are persistent, recurrent, or don’t fit a clear pattern, a CT scan allows direct visualisation of the sinus cavities and any structural abnormalities.
6. Does all facial pain have some connection to the sinuses?
No. The face contains a dense network of nerve branches, blood vessels, and joints – any of which can generate pain. Migraine, trigeminal neuralgia, and TMJ disorders all produce facial pain through entirely separate mechanisms that have nothing to do with the sinuses.