
Key Takeaways
- Children get frequent ear infections because their Eustachian tube is shorter, flatter, and more easily blocked before age five.
- Ear pulling, irritability, disturbed sleep, and fever are among the earliest warning signs parents should watch for.
- Glue ear (otitis media with effusion) causes painless, muffled hearing and is a common cause of reversible hearing loss.
- Most children have at least one ear infection before age five, with episodes declining as the tube matures by around age seven.
Dr. Sudarshen Aahire | ENT Specialist | Aahire’s ENT Superspeciality Center, Nashik
A child who won’t settle, keeps reaching for their ear, and wakes repeatedly through the night is communicating something, even without words. For parents, recognising those signals early matters enormously. Ear infections are one of the most common reasons children visit a doctor during early childhood, especially after colds or viral infections. Ear pulling, irritability, disturbed sleep, and fever are among the earliest warning signs parents should watch for.
Knowing what makes ears vulnerable, which signs to look for at different stages of a child’s development, and how a specialist can help when infections keep returning, all of this puts parents in a far stronger position to act early and protect their child’s long-term hearing and speech.
Most children experience at least one ear infection before their fifth birthday. A significant number will go through several. The goal of this guide is to help parents move from uncertainty to confident, informed action.
Why Young Children Get Ear Infections So Frequently
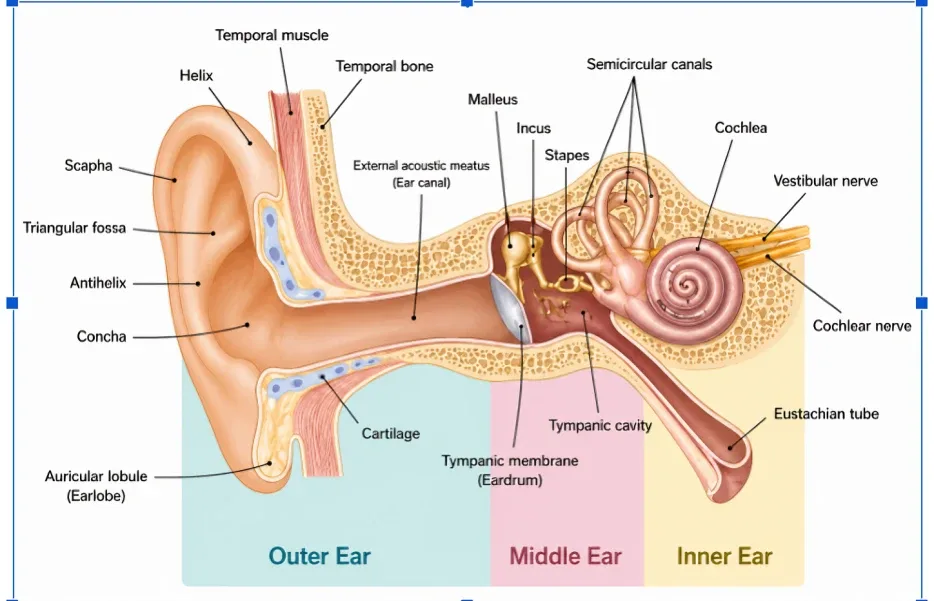
Understanding why ears are so vulnerable in early childhood comes down to one key structure: the Eustachian tube. This narrow passageway links the space behind the eardrum to the back of the throat. In a healthy ear, it drains fluid away from the middle ear and keeps air pressure balanced. In adults, the tube’s natural downward slope means drainage happens with minimal effort.
Children’s anatomy works against them here. Up to around age five, the Eustachian tube is not only shorter but runs at a much flatter angle and is made of softer, more collapsible tissue. A common cold or any upper respiratory illness can trigger enough swelling to seal this tube completely. Fluid then collects behind the eardrum with nowhere to go, creating conditions where bacteria and viruses can establish an infection rapidly.
The good news is that this vulnerability is not permanent. As a child develops, the Eustachian tube grows longer and gradually tilts downward into a more adult-like position. By around seven years of age, most children experience ear infections far less often as a direct result of this anatomical shift.
What Are The Three Main Types of Ear Infection in Children
Ear infections are not a single condition. There are three distinct forms, each with its own characteristics, and telling them apart matters for getting the right treatment.
Acute Otitis Media (AOM)
The most frequently seen form in children, AOM arrives suddenly, most often on the heels of a cold or sore throat. Infected fluid accumulates behind the eardrum, driving up pressure and causing significant pain. In some cases the eardrum perforates, releasing pus and often bringing immediate relief. With appropriate treatment, this type generally resolves fully, and any perforation typically heals without intervention.
Otitis Media with Effusion (OME) –
Glue Ear What makes glue ear difficult is its silence. After an active infection resolves, thick, sticky fluid can remain lodged in the middle ear for weeks or months, with no pain, no fever, and nothing that visibly alerts a parent. The impact, however, is real: that fluid muffles sound significantly. A child with glue ear may seem inattentive, speak at an unusually loud volume, or fail to respond when addressed from across the room. It is one of the most common causes of reversible hearing loss in the early years, and it is routinely missed.
H3-Otitis Externa, Swimmer’s Ear
This form targets the outer ear canal rather than the space behind the eardrum. Prolonged moisture, from swimming, bathing, or humid conditions, creates an environment where bacteria or fungi can take hold. The main symptoms are pain and itching within the canal, sometimes accompanied by a discharge. Unlike middle ear infections, otitis externa does not typically produce fever.
How to Recognise an Ear Infection at Every Age
The younger the child, the less directly they can communicate pain. Parents need to become fluent in the indirect signals that young children use.
Infants Under 12 Months
- Sustained crying that continues despite feeding, holding, or rocking
- Resistance or distress during feeds
- Repeated touching, batting, or grabbing at one ear
- Sleep that is far more broken than usual
- A raised temperature without another clear cause
Toddlers Aged 1 to 3
- Pulling or pressing on one ear repeatedly
- Heightened irritability and emotional swings beyond normal toddler behaviour
- Eating less or seeming uncomfortable during meals
- Waking at night after weeks or months of sleeping through
- Appearing unsteady on their feet without any obvious reason
- Inconsistent responses to their name or familiar sounds
Children Aged 3 and Older
- Verbal complaints of ear pain, fullness, or muffled sensation
- Requesting higher television volume
- Struggling to keep up in classroom settings or during group conversations
- Visible fluid at the entrance to the ear canal
Signals to Watch for Regardless of Age
- Pain or distress that worsens when the child is lying down
- Fever reaching 39°C or beyond
- Any discharge from the ear, whether watery, yellow, or blood-streaked
- A noticeable drop in hearing responsiveness
- New clumsiness or balance difficulties
- A sharp change in mood or behaviour following a recent cold
When discharge is visible, do not attempt to clean inside the ear canal. Keep it dry, and seek specialist review promptly.
What Makes Some Children More Vulnerable
While any child can develop an ear infection, several factors meaningfully raise the odds.
| Risk Factor | How It Contributes |
| Age under five | The Eustachian tube is shorter, flatter, and more easily blocked |
| Nursery or group childcare | Repeated exposure to the colds and viruses that precede ear infections |
| Lying flat during bottle feeds | Milk near the Eustachian tube opening can introduce harmful bacteria |
| Exposure to cigarette smoke | Smoke inflames the tube lining and impairs its ability to clear fluid |
| Ongoing nasal allergies | Chronic congestion keeps the Eustachian tube from draining effectively |
| Genetic tendency | Children with a family history of ear infections face higher susceptibility |
| Frequent upper respiratory infections | Colds are the most consistent trigger for middle ear infections |
When a General Practitioner Visit Is Not Enough: Signs You Need an ENT Specialist
A first or mild ear infection is usually within a General Practitioner s scope to manage. There are situations, however, where specialist evaluation becomes not just helpful but necessary, particularly when infections are repeating or when hearing is being affected.
Arrange a consultation with Dr. Sudarshen Aahire at Aahire’s ENT Superspeciality Center, Nashik if:
- Your child has had three or more ear infections within any six-month window
- Four or more episodes have occurred over the past year
- Symptoms have not improved within 48 to 72 hours of initial management
- Hearing appears reduced even after the infection has cleared
- Ear discharge persists, appears thick, or is discoloured
- Speech or language milestones are falling behind in a young child
- A glue ear diagnosis has been made and fluid has not cleared within weeks
- Infections are returning soon after finishing a course of antibiotics
Getting ahead of recurrent infections with specialist care is far preferable to managing each episode reactively. The long-term stakes – including hearing damage and speech development, make early evaluation worthwhile.
How Ear Infections in Children Are Diagnosed
An ENT specialist begins by examining the ear directly with an otoscope, which illuminates the ear canal and provides a clear view of the eardrum. A well-functioning eardrum is pale and semi-transparent; in an infected ear it is typically red, bulging, and often shows fluid collecting behind it. Where hearing loss or glue ear is a concern, further tests help complete the picture.
Tympanometry
measures how the eardrum moves in response to gentle air pressure variations. It is entirely painless and can detect trapped fluid even in a young child who cannot yet follow instructions.
Pure Tone Audiometry
is a more detailed hearing assessment for children old enough to respond to sounds. It maps any hearing reduction across a range of frequencies and guides decisions about treatment.
Nasal Endoscopy
gives the specialist a direct view of the adenoids, the soft tissue at the back of the nasal passage that frequently contributes to blocked drainage and repeated ear infections in children.
Treatment Options for Ear Infections in Children
Monitoring with Pain Management
For children over two with mild symptoms, a period of careful observation is a legitimate first step. Paracetamol or ibuprofen keeps discomfort manageable while the immune system works. Many uncomplicated infections clear without any antibiotic intervention within a few days.
Antibiotic Treatment
Antibiotics become appropriate when symptoms are assessed as severe, when the infection has spread to both ears, when the child is under two, or when there has been no meaningful improvement after 48 to 72 hours. The full prescribed course must be completed. Stopping prematurely allows infection to re-establish and is one of the contributors to antibiotic resistance.
Grommet Insertion for Glue Ear
When fluid in the middle ear persists and is demonstrably affecting hearing, grommet insertion is the recommended approach. A tiny tube is placed through the eardrum during a short procedure under general anaesthetic. This allows fluid to exit and air to return to the middle ear, with most children regaining normal hearing within days. Dr. Sudarshen Aahire performs grommet insertion as part of comprehensive paediatric ear care at Aahire’s ENT Superspeciality Center, Nashik.
Managing Root Causes
In children with enlarged adenoids or persistent nasal allergies, treatment of these underlying conditions reduces the likelihood of future infections. An ENT specialist will determine whether adenoid removal, allergy management, or a combination of both is appropriate.
What Parents Can Do at Home for Childhood Ear Infections
- Prop the child’s head slightly higher during sleep to reduce pressure behind the eardrum
- A warm flannel held gently against the ear offers short-term comfort during painful episodes
- Nothing should be inserted into the ear canal, not cotton buds, fingers, or any other object
- Removing secondhand smoke from the child’s environment has a direct, measurable effect on infection frequency
- Staying current with vaccines, particularly the pneumococcal vaccine, reduces bacterial infection risk
- Breastfeeding where possible provides immune protection that formula cannot replicate
- Always hold infants in a semi-upright position during bottle feeds, never flat
- Treating nasal congestion and allergies early prevents the chronic blockage that fuels ear infections
Why Hearing Matters So Much in These Early Years
One of the most important – and least appreciated -aspects of childhood ear infections is their potential impact on language. Children learn to speak by hearing. During the first five years, the brain is absorbing and processing spoken language at an extraordinary rate. Even mild, intermittent hearing loss during this period can quietly disrupt that process.
A child whose hearing fluctuates because of fluid-filled ears may not absorb words, sounds, and speech patterns consistently enough to develop them on schedule. Over time this can show up as limited vocabulary, unclear speech, or difficulty following instructions, not because of any fixed neurological issue, but because the input the developing brain needed was simply not arriving clearly enough.
This is the reason glue ear, despite causing no pain, is taken seriously by ENT specialists. Absence of discomfort is not the same as absence of impact. A child who cannot tell you their hearing is muffled is still being affected by it.
Key Points for Parents to Remember
- Ear infections are common in young children due to the underdeveloped structure of the Eustachian tube, this is not a reflection of poor parenting or hygiene
- Infants and toddlers cannot report ear pain; indirect cues like ear-pulling, disturbed sleep, and unusual crying are what parents need to watch
- Glue ear is painless and nearly invisible without examination, its primary impact is on hearing, not comfort
- Any pattern of three or more infections in six months calls for ENT evaluation
- Hearing disruption during the early years, even if temporary, can affect speech and learning outcomes
- Treatment is effective; with appropriate specialist input, both infections and their recurrence can be well managed
Expert ENT Care for Childhood Ear Infections
If your child is dealing with infections that keep coming back, hearing that seems inconsistent, or a recent diagnosis of glue ear that is not resolving, now is the right time to seek specialist input. The earlier an accurate diagnosis is made, the better the outcomes for hearing, speech, and overall development.
Dr. Sudarshen Aahire at Aahire’s ENT Superspeciality Center in Nashik has over 12 years of specialist experience in paediatric ear conditions, including full diagnostic assessment, grommet insertion, and adenoid evaluation. Families across Nashik trust this practice for thorough, expert care tailored to each child’s individual needs.
Frequently Asked Questions
1. How can I tell if my baby has an ear infection if they cannot speak yet?
Young children often show ear infections through behavioural changes rather than clear symptoms. Warning signs may include excessive crying, disturbed sleep, irritability during feeding, fever, or repeatedly pulling and rubbing one ear. These symptoms commonly appear after a recent cold or upper respiratory infection.
2. Are ear infections contagious between children?
The ear infection itself does not spread from one child to another. However, the cold or viral infection that triggers the ear infection can be contagious. This is why ear infections are common among children attending daycare or school environments.
3. Do all ear infections need antibiotics?
Not necessarily. Many mild ear infections, especially in children over two years of age, improve naturally within a few days. Doctors consider the child’s age, symptom severity, fever, and whether one or both ears are affected before recommending antibiotics. Persistent or worsening symptoms may require medical treatment.
4. Can ear infections cause permanent hearing problems?
Most properly treated ear infections do not lead to long-term hearing damage. However, repeated infections or long-standing glue ear can affect hearing over time if left untreated. Early diagnosis and ENT evaluation help prevent complications involving speech, hearing, and language development.
5. What are grommets and why are they used?
Grommets are tiny ventilation tubes inserted into the eardrum during a short surgical procedure. They help drain trapped fluid from the middle ear and improve air circulation. ENT specialists usually recommend grommets for children with persistent glue ear or frequent recurrent ear infections affecting hearing.
6. Will my child outgrow recurrent ear infections?
In many children, yes. As children grow, the Eustachian tube matures and drains fluid more effectively, reducing the frequency of infections. Most children experience fewer ear infections by the age of six or seven years. However, persistent infections should still be monitored carefully by an ENT specialist.
7. What should I do if fluid or discharge comes from my child’s ear?
Ear discharge should never be ignored. It may indicate pressure-related eardrum perforation caused by infection. Although pain sometimes reduces once the fluid drains, the ear still requires prompt medical assessment. Keep the ear dry and avoid inserting earbuds, oil, or other objects into the ear canal until examined by a specialist.
